Understanding Hormonal Imbalance, Metabolism, and Cycle Irregularity
At Longévité Palm Beach, we take a whole-body approach to understanding hormonal and metabolic conditions. Rather than treating symptoms in isolation, we look at the full picture: hormones, metabolism, gut health, inflammation, and lifestyle factors that influence how you feel every day.
This is where a functional medicine evaluation makes a difference.
PMOS (Polyendocrine Metabolic Ovarian Syndrome), Formerly Known as PCOS (Polycystic Ovary Syndrome)
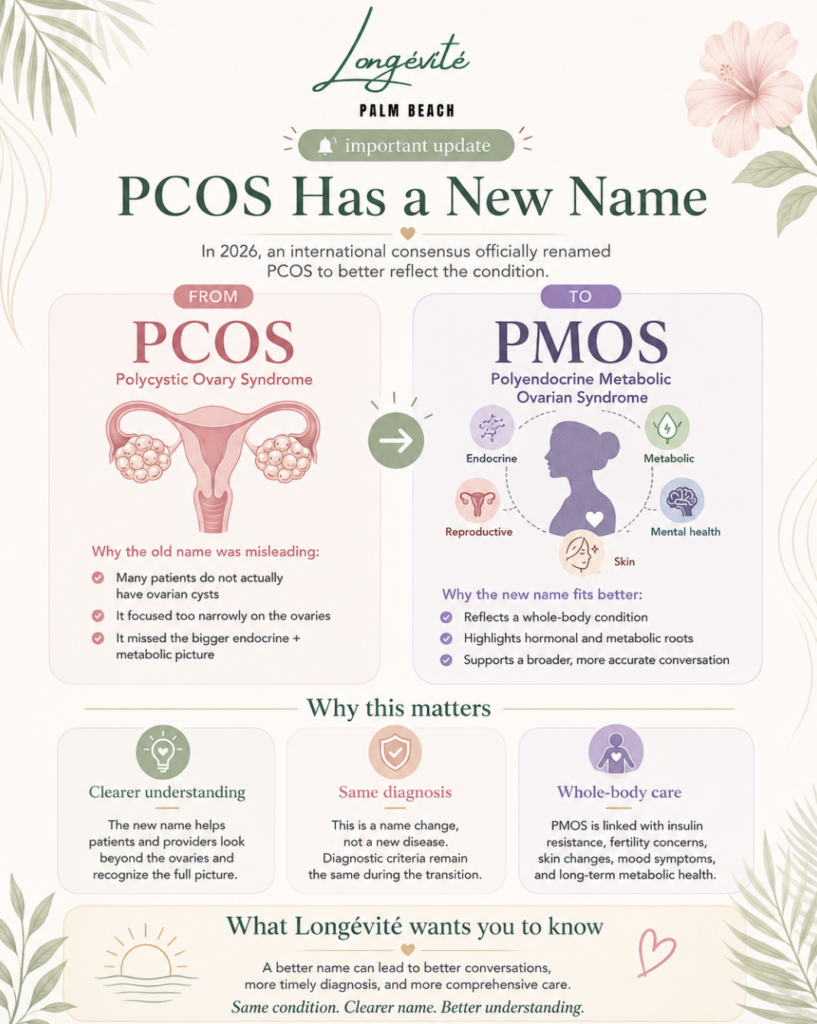
Important Update: In May 2026, an international consensus of clinicians, researchers, and patient organizations officially renamed PCOS to PMOS, Polyendocrine Metabolic Ovarian Syndrome. The diagnostic criteria remain the same. The name now reflects what practitioners like Michelle Kavall have understood for years: this is not an ovarian condition. It is a whole-body hormonal and metabolic syndrome.
If you have been diagnosed with PCOS, or suspect you might have it, nothing about your condition has changed. What has changed is how the medical community is finally talking about it.
For years, the name “polycystic ovary syndrome” led patients and providers down a narrow path. It implied cysts. It pointed at the ovaries. It framed the condition as a reproductive issue. And it missed the bigger picture that drives the symptoms most women actually struggle with: the insulin resistance, the weight that won’t move, the fatigue, the skin changes, the mood shifts, the cycle irregularities that no one could fully explain.
The new name, PMOS, corrects that. Polyendocrine means this condition involves multiple interacting hormonal systems, not just one. Metabolic acknowledges what research has confirmed for decades: insulin resistance, cardiovascular risk, and metabolic dysfunction are central features, not side effects. Ovarian keeps the reproductive component in the picture without making it the whole story.
This matters because a more accurate name leads to earlier diagnosis, better treatment, and fewer women spending years being told their symptoms are “just stress” or “normal.”
Book a Complimentary 15-Minute Consultation
Why Michelle Kavall Has Always Treated This as a Whole-Body Condition
The name change validates something Michelle has been doing in practice since she founded Longévité Palm Beach.
When a patient comes in with irregular cycles, stubborn weight gain, acne that started in her 30s, or hair changes she can’t explain, Michelle does not start with an ultrasound and stop there. She evaluates the full hormonal and metabolic landscape: androgens, estrogen, progesterone, insulin, cortisol, thyroid, inflammatory markers, and gut health. Because in her clinical experience, the patients who get the best outcomes are the ones whose providers looked beyond the ovaries.
“The old name was always a problem,” says Michelle. “It made patients think they had cysts, and it made some providers think this was only a gynecological issue. But the women sitting in front of me are dealing with insulin resistance, weight changes, energy crashes, skin issues, mood instability, and cycle disruption all at once. That is not an ovarian problem. That is a systems problem. The new name finally catches up to what we have been seeing in practice.”
Michelle Kavall, FNP-C, FMACP, is a Board-Certified Family Nurse Practitioner, Functional Medicine Specialist, and member of both the Institute for Functional Medicine and The Menopause Society. Her approach to PMOS is rooted in advanced diagnostics, personalized treatment, and ongoing clinical partnership.
Learn more about Michelle’s background and credentials
What PMOS Actually Looks Like
PMOS presents differently in every woman. Some have textbook symptoms. Others have a few overlapping concerns that no one has connected. The most common signs include:
Cycle Irregularities
Irregular, absent, or unpredictable periods. Cycles that are consistently longer than 35 days, or that come and go without pattern. Some women stop ovulating entirely without realizing it.
Metabolic and Weight Changes
Weight gain concentrated around the midsection that does not respond to conventional diet and exercise. Difficulty losing weight despite consistent effort. Blood sugar fluctuations, cravings, and energy crashes after meals. These are often driven by insulin resistance, which is present in up to 70% of women with PMOS.
Skin and Hair Changes
Acne that appears or worsens in adulthood, particularly along the jawline and chin. Thinning hair on the scalp. Increased hair growth on the face, chest, or abdomen (hirsutism). These are driven by elevated androgens, one of the hallmark hormonal imbalances in PMOS.
Fatigue and Mood Instability
Persistent low energy. Brain fog. Anxiety or depression that fluctuates with the cycle (or without a clear cycle pattern). These are downstream effects of the hormonal and metabolic dysregulation, not separate issues.
Fertility Concerns
PMOS can affect ovulation, which may impact fertility. However, many women with PMOS conceive with appropriate evaluation and support. Understanding the hormonal and metabolic picture is often the first step.
Not every woman with PMOS experiences all of these. And some women have PMOS without obvious symptoms, which is one of the reasons an estimated 70% of women with the condition are undiagnosed.
The Hormonal and Metabolic Picture Behind PMOS
PMOS is driven by the interaction of multiple hormonal and metabolic systems. Understanding these connections is what separates a surface-level diagnosis from a clinical evaluation that actually leads to resolution.
Insulin Resistance
This is the metabolic engine behind many PMOS symptoms. When cells become less responsive to insulin, the body produces more of it. Elevated insulin stimulates the ovaries to produce excess androgens, drives fat storage (particularly abdominal), disrupts ovulation, and increases inflammation. Addressing insulin resistance is often the single most impactful intervention in PMOS management, yet it is frequently overlooked in conventional care.
Androgen Imbalance
Elevated testosterone and DHEA-S are common findings in PMOS. These drive the acne, hair changes, and skin issues that many women experience. But androgens do not elevate in isolation. They are often a downstream effect of insulin resistance, adrenal dysfunction, or both. Treating the androgen excess without addressing the driver is why many conventional approaches stall.
Estrogen and Progesterone Disruption
Irregular or absent ovulation means progesterone levels drop while estrogen may accumulate. This imbalance can contribute to heavy periods, PMS, mood instability, and increased risk of endometrial changes over time.
Cortisol and Adrenal Involvement
Chronic stress and cortisol dysregulation can worsen insulin resistance, disrupt ovulation, and increase androgen production through the adrenal pathway. For women under significant stress (and in South Florida, that is a large percentage of the patient population), adrenal health is a critical piece of the PMOS evaluation.
Gut Health and Inflammation
Emerging research connects gut microbiome disruption and chronic low-grade inflammation to hormone dysregulation in PMOS. Gut health influences estrogen metabolism, insulin sensitivity, and systemic inflammation. Even in the absence of digestive symptoms, the gut may be a contributing factor.
Thyroid Connection
Thyroid dysfunction is more common in women with PMOS than in the general population. Hypothyroidism can worsen fatigue, weight gain, and cycle irregularity, and is often missed when only TSH is tested.
How PMOS Is Evaluated at Longévité
Michelle does not diagnose PMOS based on a single lab draw and an ultrasound. She evaluates the full hormonal, metabolic, and inflammatory picture to understand what is driving your specific presentation.
Testing may include:
DUTCH Testing (Dried Urine Test for Comprehensive Hormones) to assess not just hormone levels but hormone metabolism patterns, including how your body processes estrogen, progesterone, androgens, and cortisol throughout the day. DUTCH provides a level of detail that standard serum testing cannot match.
Comprehensive Metabolic and Insulin Assessment including fasting insulin, fasting glucose, HbA1c, and insulin sensitivity markers. Standard metabolic panels often miss early insulin resistance because they only flag glucose once it is already elevated. Michelle tests the insulin pathway directly.
Full Androgen Panel including total testosterone, free testosterone, DHEA-S, and sex hormone-binding globulin (SHBG). SHBG is particularly important in PMOS because low levels amplify the effects of circulating androgens even when total testosterone looks “normal.”
Complete Thyroid Panel including TSH, free T3, free T4, reverse T3, and thyroid antibodies. Not just TSH alone.
Inflammatory Markers including hs-CRP, homocysteine, and other indicators of systemic inflammation that may be driving or worsening the metabolic picture.
GI-MAP when clinical findings suggest gut health may be a contributing factor. Gut-driven inflammation and disrupted estrogen metabolism can both influence PMOS presentation.
Cortisol and Adrenal Assessment through DUTCH or salivary cortisol mapping to evaluate the stress-response pathway and its impact on insulin, ovulation, and androgen production.
Testing is guided by your symptoms, history, and clinical picture. Michelle does not run an identical panel on every patient. The goal is actionable data, not a standardized checklist.
Treatment: A Personalized, Systems-Based Approach
There is no single protocol for PMOS because there is no single cause. Treatment at Longévité is built around your specific test results, your symptoms, and the clinical findings that emerge from evaluation.
Insulin and Metabolic Support
When insulin resistance is identified, targeted intervention may include pharmaceutical support (such as metformin or newer metabolic agents when clinically appropriate), strategic nutrition changes focused on blood sugar regulation, and specific supplementation. Michelle is a licensed practitioner who can prescribe medication as part of the treatment plan.
Hormone Optimization
Based on your specific hormonal picture, treatment may include bioidentical hormone support, targeted supplementation to support progesterone production or androgen metabolism, and lifestyle strategies that influence hormone balance. Every recommendation is tied to what testing revealed, not a generic protocol.
Nutritional Strategy
When the program calls for it, Michelle brings in a Functional Nutritionist to develop a clinical nutrition plan tailored to your metabolic profile, food sensitivities, and PMOS subtype. This is not a generic “eat less sugar” recommendation. It is targeted nutrition built on lab data.
Gut Health and Inflammation Management
When gut-driven inflammation or disrupted estrogen metabolism is identified, gut restoration protocols are incorporated. This may include antimicrobials, probiotics targeted to your microbiome findings, and gut lining support.
Stress and Cortisol Management
For patients whose cortisol patterns are contributing to insulin resistance and androgen excess, adrenal support and stress-response protocols are part of the plan.
Ongoing Monitoring and Clinical Pivots
PMOS management is not a one-visit fix. Michelle monitors progress through regular check-ins and retesting when clinically indicated. If something is not producing the expected response, the plan adjusts. Retesting happens when your body’s response calls for it, not on a fixed calendar.
Book a Complimentary 15-Minute Consultation
Benefits of PMOS Evaluation and Treatment
- More regular, predictable menstrual cycles
- Improved insulin sensitivity and metabolic health
- Reduction in acne, hair thinning, and hirsutism
- Sustainable weight management supported by metabolic correction
- Improved energy, mood stability, and mental clarity
- Better understanding of fertility readiness and ovulatory patterns
- Reduced long-term cardiovascular and metabolic risk
- A clear clinical picture instead of fragmented, symptom-by-symptom care
PMOS in South Florida
South Florida’s lifestyle and environment can amplify many of the metabolic and hormonal patterns that drive PMOS.
High-stress professional lifestyles across Boca Raton, Delray Beach, and West Palm Beach create chronic cortisol elevation that worsens insulin resistance and disrupts ovulation. Dining patterns heavy in processed foods and refined carbohydrates accelerate blood sugar dysregulation. And the constant pressure to maintain a certain physique can lead to restrictive eating patterns that paradoxically worsen metabolic dysfunction.
Many women in this area have seen their OB-GYN, received a PCOS diagnosis, and been prescribed birth control or metformin without a comprehensive hormonal and metabolic evaluation. That is not wrong, but it is often incomplete. Michelle’s evaluation fills the gaps that conventional management frequently leaves open.
Longévité Palm Beach proudly serves patients via telehealth and from two locations:
Boca Raton: 561-403-1611 | West Palm Beach: 561-208-5610
H2: Frequently Asked Questions About PMOS (Formerly PCOS)
Has PCOS been renamed?
Yes. In May 2026, a global consensus of over 50 clinical, research, and patient organizations officially renamed PCOS to PMOS, Polyendocrine Metabolic Ovarian Syndrome. The Lancet published the formal name change on May 12, 2026. The diagnostic criteria have not changed. The new name more accurately reflects the condition’s hormonal and metabolic nature.
Do I need to be re-diagnosed?
No. If you have an existing PCOS diagnosis, it is now a PMOS diagnosis. The condition and the criteria are the same. Only the name has changed.
Do I need ovarian cysts to have PMOS?
No. Despite the old name, PCOS never required the presence of ovarian cysts. The “cysts” seen on ultrasound are actually arrested follicles, not pathological cysts. Diagnosis is based on a combination of symptoms, hormone patterns, and clinical findings. The new name removes this confusion.
Is PMOS only a reproductive condition?
No. This is one of the key reasons the name was changed. PMOS involves insulin resistance, metabolic dysfunction, cardiovascular risk, skin and hair changes, mood symptoms, and more. It is a multi-system condition that affects far more than the ovaries.
How is this different from what my OB-GYN does?
Most OB-GYNs focus on the reproductive aspects: cycle regulation, fertility, and ultrasound monitoring. Michelle evaluates the full hormonal and metabolic picture, including insulin resistance, cortisol patterns, thyroid function, gut health, and androgen metabolism. Her approach complements your OB-GYN’s care, it does not replace it.
Can you prescribe medication for PMOS?
Yes. Michelle is a licensed practitioner who can prescribe medication when it is clinically appropriate. This may include metformin for insulin resistance, hormone support, or other pharmaceutical interventions as part of a comprehensive treatment plan.
How long does treatment take?
It depends on your specific presentation. Some patients see improvement in energy, skin, and cycle regularity within the first few months. Metabolic correction and hormonal rebalancing are longer-term processes that typically require several months of active clinical work with regular monitoring.
Does insurance cover PMOS evaluation?
Most insurance plans do not cover the extended consultations, advanced testing (such as DUTCH testing), and ongoing monitoring that a comprehensive PMOS evaluation requires. Longévité provides superbills for out-of-network reimbursement. Many patients find the investment worthwhile because they are finally getting answers beyond “take birth control and lose weight.”
Can I still see my OB-GYN while working with you?
Absolutely. Michelle collaborates with your existing medical team. Functional evaluation of PMOS complements conventional OB-GYN care. It does not replace it.
Book a Complimentary 15-Minute Consultation
If you’re ready to understand the full picture behind your PMOS symptoms, contact Longévité Palm Beach today. Together, we’ll build a personalized plan to address the hormonal, metabolic, and inflammatory factors driving your condition.